Wales’ ambulance triage redesign shows a new approach to emergency response
In the face of mounting pressures on emergency services, the Welsh Ambulance Services NHS Trust has shifted how 999 calls are handled. Instead of automatically dispatching ambulances to the majority of calls, the trust now prioritises critical cases — where a life is at immediate risk — and assesses others through remote clinical evaluation.
This new approach reflects growing constraints on ambulance capacity and seeks to improve outcomes for the most serious emergencies while making better use of limited crews and vehicles.
Why the change matters
Ambulance demand has grown significantly post‑pandemic, stretching resources. Traditional response targets, such as reaching most calls within eight minutes, became harder to meet consistently. The Welsh trust’s strategy reframes the response model: send ambulances first where they are most likely to save lives, and for other cases use clinical triage and alternative care pathways.
The model includes several components:
Remote assessment: Callers without immediately life‑threatening conditions are evaluated by nurses or paramedics over the phone or via video. Conditions that can safely wait or be treated without an ambulance are diverted to appropriate care.
Advanced paramedics: Highly trained clinicians are deployed in cars or on bikes to assess and treat patients on site without tying up a full ambulance crew.
Digital tools: Remote monitoring applications allow patients to share vital signs with clinicians during assessment, guiding decisions on urgency.
Community responders: Volunteers and trained local responders supplement capacity for lower‑risk issues.
Implications for providers and commissioners
This shift has implications for healthcare transport and ambulance partners. Traditional metrics based on response times may evolve toward outcomes and effective use of physical resources. Providers with expertise in digital triage systems, telehealth integration, and mobile rapid response units may find new roles in the delivery ecosystem.
Workforce planning will be critical. Remote clinical assessment requires protocols and training. Investing in call‑centre clinical staff and ensuring technology supports real‑time decision‑making will be essential.
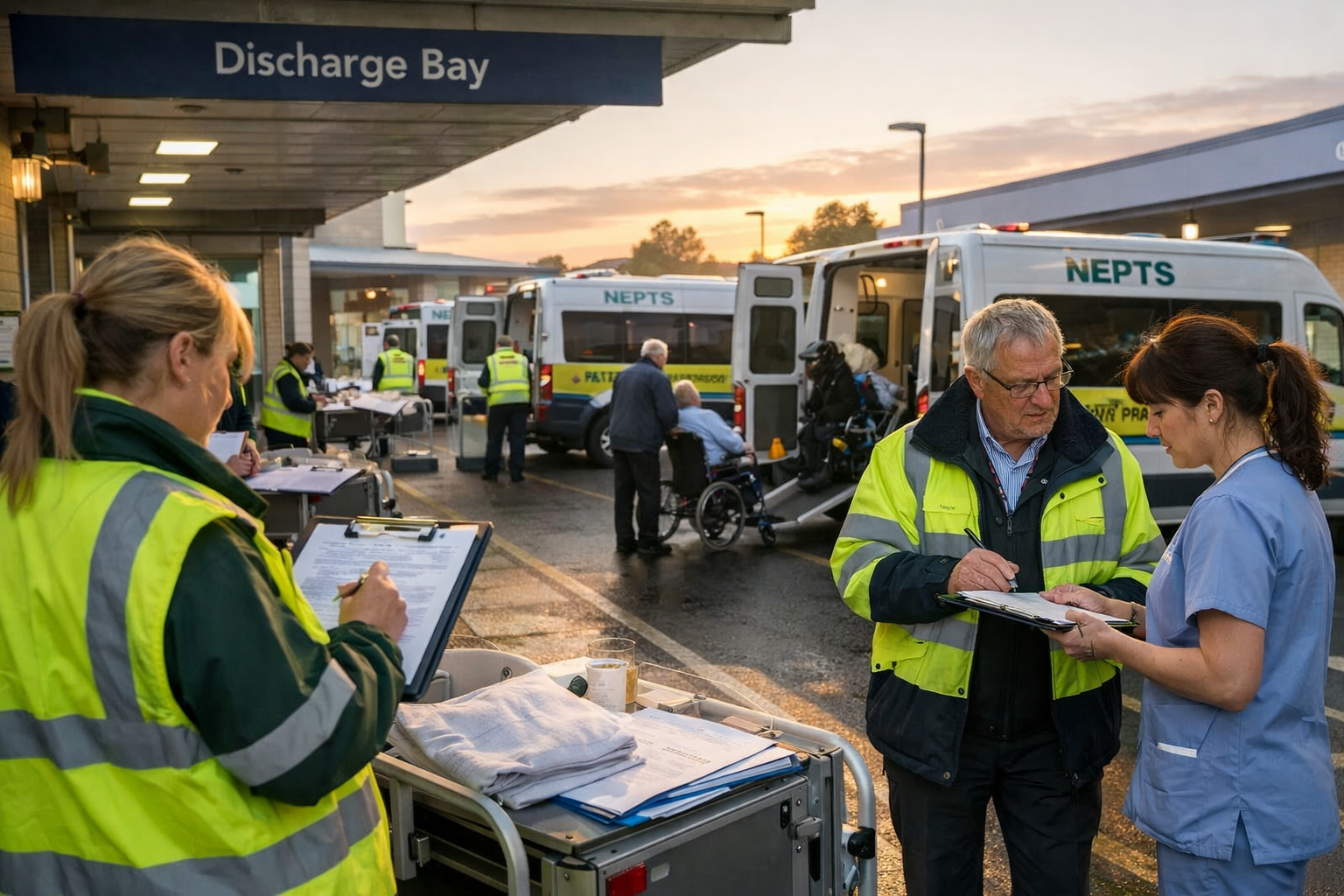
Another implication is fleet use optimisation. With ambulances reserved for the most serious cases, there may be increased demand for lower‑acuity transport or mobile care vehicles applied more efficiently. NEPTS and other patient transport systems will need to align with new demand patterns, particularly where patients are diverted from 999 to scheduled or urgent transport pathways.
What it signals about system pressures
The Welsh redesign highlights a broader issue facing NHS urgent care: balancing capacity with variable demand. As populations age and complex chronic conditions rise, demand for urgent transport and response grows. Traditional fleet expansion is expensive and slow. Adapting clinical pathways and response logic can be a practical alternative while maintaining safety.
What we learn?
Wales’ emergency response redesign represents a shift toward clinical prioritisation and efficient use of ambulances. For fleet partners and transport providers, it suggests new service models that blend digital triage, mobile response, and appropriate vehicle deployment. As this model evolves, monitoring outcomes and system effects will be key.
You might also like